One of the hot spots in the body. It is reddish brown, size of an English walnut. It can disturb one’s sleep by requiring several trips to the bathroom each night or kill a man by producing uremic poisoning. In old age it can become a site for cancer too. The prostate is a gland which contributes greatly to one’s sexual life. It is a principal storage depot for the seminal fluid, without which chances of pregnancy will be about zero. At each ejaculation, testicles provide over 150-200 million sperms cells. The prostate produces a fluid that dilutes them and this fluid contains proteins, enzymes, fats and sugars to nourish the fragile sperm, alkalinity to overcome the deadly acidity of the female tract and a watery medium in which the sperm can swim towards female egg.
It is very astonishing fact to know that the condition BPH has been explained in Ayurvedic texts long back. The anatomical position of the prostate gland, symptoms of prostate enlargement and its remedies are explained in Acharya Sushruta. The anatomical position of prostate gland is described in Ayurvedic classics as follows. In Yogaratnakara it has been described as –
“Naabheradhasthaatsanjaatha Sanchaari Yadi Vaachalaha
Ashteelaavad Ghano Granthiroodhwar Maayata Unnataha”
Which means “Below umbilicus (NAABHI), there is a hard gland which is little bit bulged and changes its place some times and some times stays stationary. This gland is like “Ashteela” (A small stone used to sharpen swords). This gland when affected by vitiated vata causes a disease called “vataashteela” (or benign prostate hypertrophy).
Sushruta explains the structure, anatomical position of prostate gland and the symptoms of prostate enlargement as follows.
“Shacranmaargasya Basheshcha Vaayurantaramaashritaha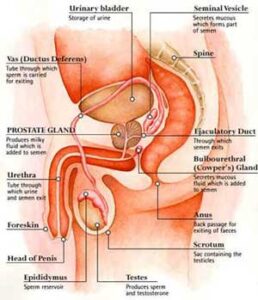
Ashteelaavadghanam Granthimmoordhvamaayata Munnatam”
Which means – the place between rectum and bladder is occupied by vitiated vata it affects the easy flow of urine, stools and se-men by enlarging the gland “ Ashteela”.
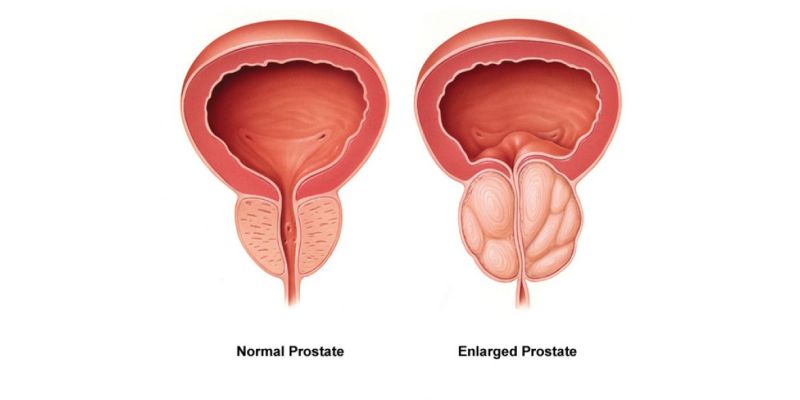
From the size of an almond in puberty, due to hormonal signals, it grows in size. It has three lobes or sections, enclosed side by side in a capsule. The small urinary tube that empties the bladder, passes over the middle lobe. Anything that happens there to swell the prostate — infection, inflammation, cancer, hypertrophy – can enlarge these lobes and thus obstruct the flow of urine , causing a wide spectrum of misery. With partial obstruction, urine backs up in the bladder and becomes a stagnant pool; bacteria often invade the pool, multiply and cause serious infection, retention, hydronephrosis etc. In an adult male, the prostate usually weighs about 20 grams. Almost all of this mass develops during puberty in response to hormonal changes associated with maturation. The prostate literally doubles in size during puberty. If a man is lucky, and some are, the prostate never again undergoes any changes in size. Unfortunately, for men between the age of 40 and 59, nearly 60% can be shown to already be suffering from benign prostatic hyperplasia (Homeopathy Treatment for Benign Prostate Hypertrophy) or prostate enlargement. This usually does not present a noticeable problem until after the age of 50. By the age of 80, however, some 85% of all men suffer from one or more symptoms of BPH. As the prostate enlarges, the layer of tissue surrounding it stops it from expanding, causing the gland to press against the urethra like a clamp on a garden hose. The bladder wall becomes thicker and irritable. The bladder begins to contract even when it contains small amounts of urine, causing more frequent urination. Eventually, the bladder weakens and loses the ability to empty itself and urine remains in the bladder. The narrowing of the urethra and partial emptying of the bladder cause many of the problems associated with prostate enlargement.
Benign prostatic hyperplasia (formerly called hypertrophy) in some ways is the male equivalent of menopause. The primary effect of BPH is a progressive decrease in the ability to empty the bladder as the prostate enlarges and applies pressure to the urethra. Retained urine from this obstruction at first can interfere with sleep as the sufferer wakes up in the middle of the night. At other times, pressure may make it impossible to properly control urine flow (incontinence). Retained urine in the bladder can allow bacterial growth and infection. Urine may flow back up the tubules to the kidneys and cause infection there. In severe cases of retention, urine even can find its way into the blood (uremia) with toxic consequences.
THEORIES FOR Prostate Enlargement
1. HORMONIC THEORY: As age advances , male hormones diminish, while estrogen does not. Tissues are enlarged due to predominance of estrogenic hormone. This is involuntary hyperplasia like fibro adenoma of breast.
2. NEOPLASTIC THEORY: Benign neoplasm. It is composed of fibrous tissues, granular tissues and muscles and is known as fibro-myo-adenoma.
PATHOLOGY:
Prostate enlargement is strongly related to normal ageing. Some of the factors involved are quite well understood. Nevertheless, there also is substantial disagreement about other issues. Prostate enlargement can be called an aspect of male menopause because an increased ratio of estrogen to testosterone is active in prostate enlargement. just as, conversely, in women passing through menopause the ratio of testosterone to estrogen increases. It is generally accepted that hormone ratios and hormone clearance are involved in prostate enlargement, but the exact ways in which these lead to the enlargement of prostate has yet to be definitively explained. Testosterone, the “male” hormone, is at its peak during adolescence. It decreases thereafter, and the rate of decrease sharpens by about age 50. The decline in testosterone production typically calls into play the compensatory release of other hormones which are stimulants to testosterone production. These cannot prevent the decline in testosterone levels, but they can lead to an elevated rate of transformation of testosterone into 5-alpha-dihydrotestosterone (DHT) and/or to the increased binding and/or to the decreased clearance of DHT from prostate cells. Testosterone is converted to DHT by the enzyme 5-alpha-reductase. Ultimately, it is DHT’s actions which cause the enlargement of the prostate. DHT binds to specific receptors on the prostate cells usually referred to as androgen receptors. It then is transported into the nucleus of these cells where it attaches to the DNA and ultimately turns on prostate growth. As will be explored in more detail below, current research indicates that DHT is a necessary, but not a sufficient cause in the etiology of BPH.
SECONDARY EFFECTS OF PROSTATIC ENLARGEMENT:
URETHRA
The portion of urethra lying above the prostate becomes elongated. Distortion of prostatic urethra .
BLADDER
Musculature of bladder hypertrophies to overcome obstruction. Urine is stagnant and may form stones. Occasionally hematuria (blood in urine)
URETER AND KIDNEY
Pressure on ureteric orifice , gradual dilation of ureter, hydronephrosis, ascending infection, nephritis
SEXUAL ORGANS
In early stages: increased sexual desireIn later stages: Impotence
Symptoms of Prostate Enlargement
FREQUENCY
§ Earliest symptom§ At first it is nocturnal§ Later: day and night§ Urgency due to stretched vesical sphincter
§ Dribbling
§ Cystitis
DYSURIA
§ Patient must wait for urination to start§ Useless to strain
STREAM
§ Variable§ Weak§ Tends to stop§ Starts and dribbles
PAIN
§ Only due to cystitis or acute retention of urine
§ May be dull
§ Feeling of fullness in lower abdomen
RETENTION
§ Acute retention of urine
§ Retention with overflow, constant dribbling
URINE
§ Occasional Haematuria
KIDNEY
§ Renal insufficiency
EXAMINATION
RENAL AREA
Tender
TONGUE
Brown, dry
RECTAL EXAMINATION
§ Absence of full bladder§ Bimanual : Dorsal position : the enlargement can be felt
BLOOD
- Blood urea increased, ESR increased
- Prostate-specific antigen (PSA): It is a protein produced by the cells of the prostate gland. The PSA test measures the level of PSA in the blood. The doctor takes a blood sample, and the amount of PSA is measured in a laboratory. Because PSA is produced by the body and can be used to detect disease, it is sometimes called a biological marker or tumor marker. It is normal for men to have low levels of PSA in their blood; however, prostate cancer or benign (not cancerous) conditions can increase PSA levels. As men age, both benign prostate conditions and prostate cancer become more frequent. The most common benign prostate conditions are prostatitis (inflammation of the prostate) and benign prostatic hyperplasia (BPH) (enlargement of the prostate). There is no evidence that prostatitis or BPH cause cancer, but it is possible for a man to have one or both of these conditions and to develop prostate cancer as well. PSA levels alone do not give doctors enough information to distinguish between benign prostate conditions and cancer. However, the doctor will take the result of the PSA test into account when deciding whether to check further for signs of prostate cancer.
PSA test results report the level of PSA detected in the blood. The test results are usually reported as nanograms of PSA per milliliter (ng/ml) of blood. In the past, most doctors considered PSA values below 4.0 ng/ml as normal. However, recent research found prostate cancer in men with PSA levels below 4.0 ng/ml (2). Many doctors are now using the following ranges, with some variation:
o 0 to 2.5 ng/ml is low
o 2.6 to 10 ng/ml is slightly to moderately elevated
o 10 to 19.9 ng/ml is moderately elevated
o 20 ng/ml or more is significantly elevated
IVU
The shape and position of urethra will help in diagnosing, contraindicated in case of renal insufficiency
URINE FLOW STUDY
Sometimes the patient is asked to urinate into a special device that measures how quickly the urine is flowing. A reduced flow often suggests prostate enlargement.
OTHER
CYSTOURETHROSCOPY, ULTRA SONOGRAPHY
COMPLICATIONS of Prostate Enlargement
- Acute Retention
- Chronic Retention: The bladder is not completely emptied after passing urine. Some urine remains in the bladder at all times. This is called ‘chronic (ongoing) retention’. This may cause recurring urine infections, or incontinence (as urine dribbles around the blockage rather than large amounts being passed each time patient goes to the toilet).
- Infection
- Uremia
- Hydronephrosis
- Renal Failure
INDICATION FOR OPERATION
§ Dysuria
§ Acute retention
§ Chronic retention
§ Complications: stone, infections
§ Hemorrhage
TREATMENT
- Catheterization: In case of retention of urine
- Transurethral microwave procedures. Prostatron, a device that uses microwaves to heat and destroy excess prostate tissue. In the procedure called transurethral microwave thermotherapy (TUMT), the Prostatron sends computer-regulated microwaves through a catheter to heat selected portions of the prostate to at least 111 degrees Fahrenheit. A cooling system protects the urinary tract during the procedure. Although microwave therapy does not cure BPH, it reduces urinary frequency, urgency, straining, and intermittent flow. It does not correct the problem of incomplete emptying of the bladder. Ongoing research will determine any long-term effects of microwave therapy and who might benefit most from this therapy.
- Transurethral needle ablation. Transurethral Needle Ablation (TUNA) System for the treatment of BPH. The TUNA System delivers low-level radiofrequency energy through twin needles to burn away a well-defined region of the enlarged prostate. Shields protect the urethra from heat damage. The TUNA System improves urine flow and relieves symptoms with fewer side effects when compared with transurethral resection of the prostate (TURP). No incontinence or impotence has been observed
- Transurethral surgery. A procedure called TURP (transurethral resection of the prostate) is used for 90 percent of all prostate surgeries done for BPH. With TURP, an instrument called a resectoscope is inserted through the penis. The resectoscope, which is about 12 inches long and 1/2 inch in diameter, contains a light, valves for controlling irrigating fluid, and an electrical loop that cuts tissue and seals blood vessels. The surgeon uses the resectoscope’s wire loop to remove the obstructing tissue one piece at a time. The pieces of tissue are carried by the fluid into the bladder and then flushed out at the end of the operation. Transurethral procedures are less traumatic than open forms of surgery and require a shorter recovery period.
- Prostectomy . In the few cases when a transurethral procedure cannot be used, open surgery, which requires an external incision, may be used. Open surgery is often done when the gland is greatly enlarged, when there are complicating factors, or when the bladder has been damaged and needs to be repaired. The location of the enlargement within the gland and the patient’s general health help the surgeon decide which of the three open procedures to use.
- Laser surgery. In March 1996, FDA approved a surgical procedure that employs side-firing laser fibers and Nd: YAG lasers to vaporize obstructing prostate tissue. The doctor passes the laser fiber through the urethra into the prostate using a cystoscope and then delivers several bursts of energy lasting 30 to 60 seconds. The laser energy destroys prostate tissue and causes shrinkage. Like TURP, laser surgery requires anesthesia and a hospital stay. One advantage of laser surgery over TURP is that laser surgery causes little blood loss. Laser surgery also allows for a quicker recovery time. But laser surgery may not be effective on larger prostates. The long-term effectiveness of laser surgery is not known.
PROSTATE SELF CARE
Making some lifestyle changes can often help control the symptoms of an enlarged prostate and prevent the condition from worsening. The patient should be advised the following:-
o Limit beverages in the evening. Stop drinking water and other beverages after 7 p.m. to reduce need to go to the bathroom at night. In particular, beverages that contain caffeine will increase urine production, cause bladder irritation and aggravate the symptoms.
o Empty the bladder. Avoid letting the bladder get full. Try to urinate all that he can each time he goes to the bathroom. For some men, sitting on the toilet is more effective than standing. Try following a daily time schedule for urinating, such as on long trips.
o Limit alcohol. Alcohol increases urine production and irritates the bladder.
o Be careful with over-the-counter decongestants. They can cause the band of muscles that control urine flow from the urethra (urethral sphincter) to tighten, making urination more difficult.
o Keep active. Inactivity causes bladder to retain urine. Even a small amount of exercise can reduce urinary problems caused by an enlarged prostate.
Stay warm. Cold weather can lead to urine retention and increase your urgency.
HOMEOPATHIC TREATMENT for Enlarged Prostate
As is obvious, any patient must be treated on its individuality and not on the disease symptoms. BPH is a condition, which may mislead any physician due to dominance of disease symptoms taking priority in the hands of patient. He is so disturbed, so embarrassed that he will sometimes not give importance to his particular, uncommon peculiar and constitutional symptoms. It is prudent for a physician to take some symptoms for relief of the patient as palliative measure but if he wants to give him permanent or long lasting relief, a proper prescription on the basis of miasm, constitution, individuality, general and particular symptoms is important. Sycosis plays an important part in this disease whereas overall mixed miasm may be found in patients.
Commonly indicated homeopathy medicines for BPH
- Sabal serrulata ( saw palmetto)
- Thuja occidentalis ( arbor vitae )
- Petroselinum ( parsley )
- Hydrangea ( seven barks )
- Solidago virga (golden rod)
- Prunus spinosa (black thorn)
- Ferrum picricum (picrate of iron)
- Cantharis (spanish fly)
- Conium maculatum
- Staphysagria
- Arnica Montana
- Phosphorous
- Iodum
- Arsenic iod
- Baryta carb
- Pareira Brava
- Belladonna
- Digitalis
I would like to describe as therapeutics for a case of BPH depending on the Physiological action, natural ingredients and clinical proving. Some of the most important medicines are as follows:-
SABAL SERRULATA ( SAW PALMETTO)
Recently, medical literature has provided increased support for the use of naturally occurring nutrients that prevent the progressive enlargement of the prostate gland (BPH). Some of these nutrients have even been demonstrated to reduce the incidence of prostate cancer! These nutrients that combat the detrimental effects of DHT in the prostate can be utilized to combat the effects of DHT in hair loss. The following discussion outlines multiple DHT fighting agents.
This is by far the most commonly recognized and discussed herb concerning the prostate. Saw palmetto is a plant (dwarf palm tree) native to the United States. It has been used medicinally for over a century with its first use being described in the medical literature in the 1800s. Early literature concerning saw palmetto described it as relieving symptoms ranging from prostate enlargement in men to gynecological problems in women such as menstrual discomfort. Most of the substances found to be effective in treating benign prostatic enlargement are found in the extract form. The extract form has been demonstrated to be more potent than the dried berry form. The active constituents are volatile oil, steroidal saponin, tannins, and polysaccharides. Saw Palmetto is one of the few herbal products that is considered to be anabolic – it strengthens and builds body tissues. For men it treats an enlarged and weakened prostate gland. It has shown significant action in treatment of conditions associated with benign prostatic hypertrophy (BPH). Saw palmetto extract works to prevent testosterone from converting into dihydrotestosterone, the hormone thought to cause prostrate cells to multiply leading to an enlarged prostate, and to increase male & female pattern baldness. It is chiefly used as a diuretic and to tone the bladder by improving urinary flow, and relieving strain. Regular use of saw palmetto may decrease urinary frequency, especially during the night, by allowing complete bladder expulsion and reducing inflammation of the bladder and enlarged prostrate. Saw palmetto inhibits androgen and estrogen receptor activity and may be beneficial for both sexes in balancing the hormones and stimulating healthy hair growth. Saw palmetto helps reduce high Dihydro-testosterone (DHT) levels in the blood which can seriously damage hair follicle growth and is the main cause of pattern baldness. Because of it’s hormonal effect it can aid the thyroid in regulating sexual development and normalizing activity of those glands and organs.
§ Unquestionable importance in prostate enlargement
§ Constant desire to urinate < night
§ Enuresis
§ Paresis of sphincter vesicae
§ Dysuria
§ Cystitis
§ Acts on membrano-prostatic part of urethra
THUJA OCCIDENTALIS ( ARBOR VITAE )
§ Acts on genito urinary tract producing sycotic dyscrasia.
§ Sycotic pains: pain muscles and joints
§ Hydrogenoid constitution
§ Rapid emaciation and exhaustion
§ Fixed ideas: as if a strange person is at his side, as if soul and body were separated, as if something alive were in abdomen
§ Enlarged prostate
§ History of gonorrhoea
§ Inflammation of glans and prepuce
§ Gonorrheal rheumatism
§ Swelling of urethra with split stream
§ Sensation of tickling in urethra after urinating
§ Desire sudden and urgent, can not be controlled
§ Frequent desire to urinate
§ Pain lower abdomen
PETROSELINUM ( PARSLEY )
Parsley is native to the Mediterranean region of Southern Europe. While it has been cultivated for more than 2,000 years, parsley was used medicinally prior to being consumed as a food. The ancient Greeks held parsley to be sacred, using it to not only adorn victors of athletic contests, but also for decorating the tombs of the deceased. The practice of using parsley as a garnish actually has a long history that can be traced back to the civilization of the ancient Romans. The flavonoids in parsley – especially luteolin – have been shown to function as anti-oxidants that combine with highly reactive oxygen-containing molecules (called oxygen radicals) and help prevent oxygen-based damage to cells. In addition, extracts from parsley have been used in animal studies to help increase the anti-oxidant capacity of the blood.
§ Burning , tingling from perineum throughout urethra
§ Sudden urging to urinate
§ Sudden irresistible desire to urinate
§ Intense, biting, itching, deep in urethra
§ Milky discharge
§ Associated with piles
HYDRANGEA ( SEVEN BARKS )
Hydrangea has been used for hundreds of years as a treatment for enlarged or inflamed prostate glands, and is often combined with Horsetail for this purpose. It is one of the best herbal remedies for treatment of pain related to kidney problems, especially kidney stones, by reducing the size of the stones and allowing them to pass painlessly. In Greek mythology, Hydra was a water monster with nine heads, and if one was cut off, the monster grew back two. A water “hydrant” also helps remind us that hydrangea has to do with the body’s water. Hydrangea is very high in silicon, needed to maintain flexible arteries, especially important for good blood circulation through the filtering tubules of each kidney. Manganese has only been appreciated the last few years in its ability to strengthen nerves, the immune system, digestion of fats, blood sugar regulation, growth and reproduction. These factors also impact demands on the urinary system. Also found naturally in relatively large amounts is chromium, essential for proper blood sugar levels and circulatory health.
§ Enlargement of prostate
§ Remedy for stones, profuse deposits of white amorphous salts in urine
§ Burning in urethra and frequent desire
§ Urine hard to start
§ Sharp pains in loins
§ Enlarged prostate with great thirst
SOLIDAGO VIRGA (GOLDEN ROD)
§ Pain in region of Kidneys, with dysuria
§ Kidneys sensitive to pressure
§ Difficult and scanty urine
§ Makes the use of catheter unnecessary
§ Associated with calculus
§ Kidney and urinary symptoms are more marked
§ Used when cystitis and kidney affections are present with BPH
§ Reddish brown urine with thick sediments
§ Pain in kidneys , extending to abdomen and bladder
§ Clear and offensive urine
§ Very helpful in case of retention, makes the use of the catheter unnecessary at times.
PRUNUS SPINOSA (BLACK THORN)
§ PROSTATE enlargement with retention symptoms
§ Hurriedly impelled to urinate
§ The urine seems to pass as far as the glans and then returns and causes pain in urethra
§ Tenesmus of bladder
§ Useful in retention symptoms where patient has to press a long time before urine passes
§ Neuralgic dysuria
§ Associated with ciliary neuralgias, left sided
§ Ineffectual urge to urinate
§ Dropsy and anasarca
FERRUM PICRICUM (PICRATE OF IRON)
§ One of the best medicine for senile prostatic hypertrophy or enlarged prostate in old men.
§ Good medicine to complete the action of other medicines (Boericke)
§ Frequent micturition at night
§ Full feeling and pressure in rectum
§ Retention of Urine
§ Smarting at neck of bladder
CANTHARIS (SPANISH FLY)
The Cantharis vesicatoria, or Lytta vesicatoria as the beetle is called nowadays is widely known under its popular name Spanish Fly. Many of us know that this little creature is used in love-potions to stimulate sexual arousal. Cantharidine taken in large doses is poisonous; it causes vomiting and burning pain of the urinary track, which shows in its symptomatology.
§ One of the best medicine for prostate enlargement with burning urination
§ Burning pain and an intolerable, constant urge to urinate while only losing a few drops of urine
§ All pains are sore, raw, burning, cutting, biting and smarting.
§ Intense sexual desire arises from the inflamed pelvic region..
§ The urge to urinate is intolerable and constant; before, during and after the painful urination.
§ Only a few bloody drops will pass at a time and the pain in the urethra and bladder are intense burning, cutting and itching.
§ Symptoms get worse by drinking of water or coffee, urination, glittering objects, the sound of water. The person feels better by warmth, rubbing and massage.
I have not necessarily covered all medicines, but this is my humble effort to make the therapeutics slightly easier to help students, teachers and physicians to deal with a very common problem of modern age.
EXTRA SHOTS
International Prostate Symptom Score (IPSS)
International Prostate Symptom Score (IPSS): Developed to quantitate and validate responses to the questions asked, this set of 7 questions has been adopted worldwide and yields reproducible and quantifiable information regarding symptoms and response to treatment. Each question allows the patient to chose 1 of 6 answers indicating increasing severity of symptoms on a scale of 0-5; the total score ranges from 0-35. Questions concern incomplete emptying, frequency, intermittency, urgency, weak stream, straining, and nocturia. The eighth question is known as the bother score and pertains to the patient’s perceived QOL. Scores can range from 0 (delighted) to 6 (terrible). After calculating the total score for all 8 eight questions, patients are classified as 0-7 (mildly symptomatic), 8-19 (moderately symptomatic), or 20-35 (severely symptomatic). Specific IPSS questions are as follows (adapted from the recommendations of the International Scientific Committee, 2000):
1. Incomplete emptying: Over the past month, how often have you had the sensation of not emptying your bladder completely after you have finished urinating? (Not at all = 0, less than 1 time in 5 = 1, less than half the time = 2, about half the time = 3, more than half the time = 4, almost always = 5)
2. Frequency: Over the past month, how often have you had to urinate again less than 2 hours after you finished urinating? (Not at all = 0, less than 1 time in 5 = 1, less than half the time = 2, about half the time = 3, more than half the time = 4, almost always = 5)
3. Intermittency: Over the past month, how often have you stopped and started again several times when urinating? (Not at all = 0, less than 1 time in 5 = 1, less than half the time = 2, about half the time = 3, more than half the time = 4, almost always = 5)
4. Urgency: Over the past month, how often have you found it difficult to postpone urination? (Not at all = 0, less than 1 time in 5 = 1, less than half the time = 2, about half the time = 3, more than half the time = 4, almost always = 5)
5. Weak stream: Over the past month, how often have you had a weak urinary stream? (Not at all = 0, less than 1 time in 5 = 1, less than half the time = 2, about half the time = 3, more than half the time = 4, almost always = 5)
6. Straining: Over the past month, how often have you had to push or strain to begin urination? (Never = 0, once = 1, twice = 2, thrice = 3, 4 times or more = 4, 5 times or more = 5)
7. Nocturia: Over the past month, how many times did you most typically get up to urinate from the time you went to bed until the time you got up in the morning? (Not at all = 0, less than 1 time in 5 = 1, less than half the time = 2, about half the time = 3, more than half the time = 4, almost always = 5)
Bother score: This helps assess perceived QOL due to urinary symptoms, and the score ranges from 0 (delighted) to 6 (terrible). How would you feel if you were to spend the rest of your life with your urinary condition just the way it is now? (Delighted = 0, pleased = 1, mostly satisfied = 2, mixed = 3, mostly dissatisfied = 4, unhappy = 5, terrible = 6)
Prostate Enlargement – Symptoms, Treatment, Surgery, Cure and Homeo Treatment or Homeopathy remedies for enlarged prostate.
BIBLIOGRAPHY
1. KNOW YOUR BODY: READER’S DIGEST
2. HOMOEOPATHIC MAT. MEDICA: KENT, FARRINGTON & WILLIUM BOERICKE


I find this one of the best papers covering treatment of BPH.
Reading this provided me a complete knowledge about the most common ailments that we, men suffers and understanding the history as laid down by Dr. Singh is remarkable, precise and complete. Kudos to you Dr. Singh!
My question: What is the best Homeopathic remedy for this malady? How do you rate Prostonum drops?
Can Bayta Carb 30c and Conium 30c be taken together?
Can Prostonum be taken in association with Baryta Carb and Conium?
Appreciate your kindness and deep concern for us men.
Kindest regards,
Arthur J. Millare
WHAT IS MEDICNE IF PROSTATE IS LARGE AND ICHIING START