
Are you looking for a homeopathic cure for appendicitis? This article discusses the homeopathy treatment of appendicitis along with the best homeopathic medicine for appendicitis treatment.
What is Appendicitis?
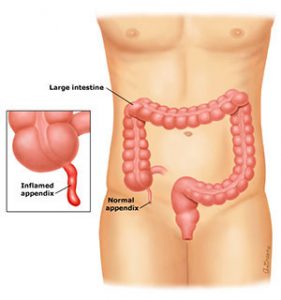 Appendicitis is a term which is used for “inflammation of the appendix”, a small tube of tissue that connects to the beginning of the large intestine, usually at the lower right side of the abdomen. Appendicitis is the most common reason for emergency abdominal surgery.
Appendicitis is a term which is used for “inflammation of the appendix”, a small tube of tissue that connects to the beginning of the large intestine, usually at the lower right side of the abdomen. Appendicitis is the most common reason for emergency abdominal surgery.
People who have family history of appendicitis are at an increased risk of developing appendicitis. If this condition is not treated properly on time, it can lead to severe complications.
- Due to the commonly ambiguous presentation, the diagnosis is often initially missed
- Very young and very old patients are more likely to have an atypical presentation; thus a much lower threshold for pursuing the diagnosis is necessary.
- Despite advances in imaging, the rate of negative appendectomies (appendicitis not the cause of symptoms) has not changed in the last two decades (roughly 15-20%)
- Morbidity is low given its prevalence among young, healthy people; however, when not treated appropriately, it remains a potentially lethal condition.
Homeopathy Treatment of Appendicitis

Homeopathy is one of the most popular holistic systems of medicine. The selection of homeopathic medicine for appendicitis is based upon the theory of individualization and symptoms similarity by using holistic approach.
This is the only way through which a state of complete health can be regained by removing all the sign and symptoms from which the patient is suffering.
The aim of homeopathic medicine for appendicitis is not only to treat appendicitis but to address its underlying cause and individual susceptibility. As far as therapeutic medication is concerned, several remedies are available to treat appendicitis that can be selected on the basis of cause, sensations and modalities of the complaints.
For individualized homeopathic medicine for appendicitis and treatment, the patient should consult a qualified homeopathic doctor in person. There are following remedies which are helpful in the treatment of appendicitis:
Belladonna
- Indicated in early stage of inflammation.
- Patient is very sensitive to pain touch, noise etc.
- Fever with appendicitis.
- Slightest jar increases the pain.
- Pain aggravated by coughing, sneezing & touching.
- Pain as if clutched by a hand.
- Dryness of mouth and throat with aversion to drink.
Bryonia alba
- The general character of the pain here produced is a stitching, tearing; worse by motion, better rest. These
 characteristic stitching pains, greatly aggravated by any motion
characteristic stitching pains, greatly aggravated by any motion - The Bryonia patient is irritable; has vertigo from raising the head.
- Pressive headache; dry, parched lips, mouth; excessive thirst, bitter taste,
- Sensitive epigastrium, and feeling of a stone in the stomach;
- Stools large, dry, hard
- Tenderness of abdominal walls.Burning pain, stitches; worse, pressure, coughing, breathing.
 characteristic stitching pains, greatly aggravated by any motion
characteristic stitching pains, greatly aggravated by any motionArsenicum album
- Great exhaustion after the slightest exertion.
- Burning pains. Unquenchable thirst. Burning relieved by heat.
- Great anguish and restlessness. Changes place continually.
- Fears, of death, of being left alone. Great fear, with cold sweat. Thinks it useless to take medicine.
- Abdomen swollen and painful. Pain as from a wound in abdomen on coughing.
Rhus toxicodendron
- Extreme restlessness, with continued change of position.
- Violent pains in abdomen, relieved by lying on abdomen.
- Swelling of inguinal glands.
- Pain in region of ascending colon. Colic, compelling to walk bent.
- Excessive distension after eating
- Nausea, vertigo, and bloated abdomen after eating
Lachesis
- Abdomen tympanitic, sensitive, painful.
- Constipated, offensive stool.
- Hot perspiration, bluish, purplish appearance.
- Patient sleeps into an aggravation.
- Very important during the climacteric and for patients of a melancholic disposition.
Sulphur –
- Should be used as a intercurrent remedy to complete the cure.
Iris tenax –
- Well known remedy for appendicitis; pain in the ileo-caecal region, extreme tenderness on pressure.
Dioscorea –
- Constant pain; bowels filled with gas; pain of gripping character; twisted pain ameliorated by bending backward.
Colocynth –
- Indicated when there is intense cutting, cramping or twisting pain; which is worse by indigestion and relieved by warmth, and pressure.
Ignatia –
- Body hot and rigid; extreme pain in the region of appendix with fear of getting operated; patient is much sensitive, alert with great nervous feeling.
Mercurius –
- Acts well on acute condition; swelling hard hot and painful in ileo-caecal region; tender lump felt in the region of appendix.
Cause of Appendicitis
Appendicitis is an inflammation of the appendix, the main cause of appendicitis is blockage of opening of appendix by mucus or fecal material (stool). Other causes mainly include infection by bacteria and swelling of lymphatic tissue within the appendix.
- Lumen obstruction is thought to be the inciting event leading to inflammation and infection of the appendix; obstruction is most commonly caused by a fecalith, which results from accumulation and inspissations of fecal matter.
- Other causes include neoplasms, foreign objects, and enlarged lymphoid follicles
- Obstruction of the lumen leads to distention, increased intraluminal pressure, venous engorgement, impaired arterial blood supply, and ischemia.
- As the ischemic, mucosal barrier breaks down, bacterial invasion from the colon occurs resulting in inflammation, necrosis, and rupture.
- Histologically, obstruction is indentified in only 30-40% of cases; potential causes in the absence of luminal obstruction include mucosal ulceration due to the infection.
- Cultures reflect colonic flora pathogens and are always polymicrobial: Anaerobic Streptococci, Enterobacter, Bacteroides, Prevotella, and other gram-negative anaerobes
- The higher incidence occurs in the 10 to 19 years old age group
- 10% of the U.S. population will develop appendicitis at some time in their lives
- It is the most common general surgical disorder during pregnancy, affecting up to 0.1%
Symptoms of Appendicitis
- The classic presentations is 12-48 hours of progressive, diffuse, crampy pain that localizes to the right lower quadrant (McBurney point) and becomes a sharp pain
- A history of pain preceding nausea and or emesis has nearly 100% sensitivity for appendicitis
- Atypical findings (e.g. dysria, tenismus) are often found in children, the elderly, and patients with a retrocecal appendix
- Low grade fever is common; high fever should raise suspicion of perforation or another diagnosis
Early symptoms of appendicitis
- Spasmodic or gripping abdominal colic which is off and on in character (comes and goes)
- Anorexia or loss of appetite
- Hard stools or constipation
Late symptoms of appendicitis mainly involves
- Intense pain in right iliac region (right lower abdomen), which may move up or down from umbilicus.
- Nausea
- Vomiting
- Increased temperature
- Increased pulse rate
- Sometimes patient may have diarrhea
- Patient feels amelioration when bend the right leg up, stretching it down aggravates pain.
Signs of appendicitis
Cough tenderness – this is an important sign which differentiate appendicitis from right sided ureteric colic.
Cope’s psoas test – irritation of psoas major muscle which produces flexion at the hip, any attempt of extension causes pain. Right lower quadrant pain upon passive extension of right leg
Cope’s obturator test – irritation of the obturator muscle, flexion and medical rotation causes pain. Right lower quadrant pain upon passive internal rotation of flexed leg.
Tenderness and rebound tenderness – present at Mc Burney’s point. Rebound tenderness is due to inflammation of the partial peritoneum.
Guarding and rigidity – in the right ileac fossa
Roving sign (referred rebound tenderness) – palpation of left ileac region of abdomen producing pain in the right iliac region.
Differential diagnosis of appendicitis
- Acute pancreatitis
- Enterocolitis
- Meckel’s diverticulitis
- Acute cholecystitis
- Right sided ureteric colic
- Torsion of undescended testes
- Perforated duodenal ulcer
In females:
- Torsion of ovarian cyst
- Bilateral Salpingooophoritis
- Ruptures ectopic gestation
- Mid menstrual rupture of ovarian follicle
Differential Diagnosis by Organ
- Small bowel: Meckel’S diverticulitis, Crohn’s, disease, small bowel obstruction, gastroenteritis
- Colon: Colon cancer, cecal diverticulitis, ulcerative colitis bacterial ileitis ( Y. enterocolitica or C. jejuni), amebic or tuberculous colitis, constipation
- Genitourinary: Cystitis, pyelonephritis, nephrolithiasis
- Gynecologic: Mittelschmerz, salpingitis, tubo-ovarian abscess, ovarian torsion, ovarian cyst rupture, ectopic pregnancy
- Other: Mesenteric adenitis, right lower lobe pneumonia, referred hip pain
Diagnosis of Appendicitis
1. History and physical exam generally suggest the diagnosis
- No single sign or symptom reliably establishes the diagnosis
- About 20% of diagnoses are missed
- Low -grade fever is common; high fever should raise suspicion of
- perforation or another diagnosis
- A pelvic exam should be performed in all women of reproductive age
2. Laboratory testing includes complete blood count, urinalysis, and pregnancy testing
- Complete blood count generally reveals mild leucocytosis but is normal in 30% of patients; 95% of patients have a left-shift ( increased immature white blood cells)
- Urinalysis should be normal; pyuria can result from appendiceal irritation of ureter.
- Urine pregnancy testing is necessary in all females of reproductive age to rule out pregnancy; however, a positive pregnancy test does not rule out appendicitis
3. Diagnosis should not require imaging on otherwise healthy patients with straightforward clinical presentations; however, CT scan is becoming a routine means of diagnosis
- Abdominal and pelvic CT scans with contrast are especially useful in patients with atypical presentation (e.g. retrocecal appendix) and to rule out appendiceal abscess
- CT scan has sensitivity of 95- 98% and specificity of 80-90% for appendicitis
4. Ultrasound may visualize an inflamed appendix and is useful to evaluate gynecologic diagnoses; however, a normal ultrasound does not exclude appendicitis
5. Immediate surgical consultation (prior to imaging) is warranted if high suspicion exists
Treatment of Appendicitis
Appendicitis is treated by removal of the appendix through appendectomy (a surgical procedure to remove appendix.) It involves open surgical incision in the right lower portion of the abdomen. This can be done through laparoscopy in which a small incision is given and during whole procedure a camera visualize the area of interest.
Antibiotic treatment is often given prior to surgical operation to reduce inflammation and to kill remaining bacteria.
PROGNOSIS & COMPLICATIONS
- Mortality is rate but is increased in very young (<years) and very old patients
- Rapid recovery and low mortality with early diagnosis and treatment
- The most common postoperative complications include superficial wound infection (5%) and intra-abdominal abscess (2%), which generally requires surgical drainage
- Rupture and/ or peritonitis may also occur, which require repeat operations and generally result in a prolonged recovery
- Fever exceeding 103°F and elevated white blood cell count are more likely in cases of perforation
- Perforation and subsequent abscess formation are more likely if symptoms have been ongoing for more than 48-72 hours.
Note: The above homeopathy medicines are just an indicator of how we can treat appendicitis with homeopathy. Please consult a qualified homeopath in person for a full case analysis and to find the best homeopathy remedy for your individual case.
Appendicitis Cases Cured With Homeopathic Medicine
A Case of Acute Appendicitis – by Krutik Shah
A Case of Acute Appendicitis – by S. Arul Manickam
Appendicitis Complicated with Abscess In a 9 Year Old Boy with Achondroplasia – by Corina Butiu
A Case of Vesico-Ureteric Reflux – by Sanjay Padole

Sir we have a apendix patients which are served severe pain
So guide me